What is Carpal Tunnel Syndrome?
Carpal tunnel syndrome (CTS) is one of the most common nerve compression conditions affecting the upper extremity. It is characterized by pressure on the median nerve as it passes through the carpal tunnel at the wrist, resulting in pain, numbness, tingling, and — in advanced cases — permanent loss of hand function. This page provides a comprehensive clinical overview of CTS, including anatomy, causes, symptoms, diagnostic methods, and all available treatment options. For a broader introduction to the condition, see our Understanding CTS page.
Brandon P. Donnelly, MD is a board-certified orthopedic surgeon specializing in hand and upper extremity conditions, serving patients throughout the Greater New Orleans area. For answers to frequently asked questions, visit our Carpal Tunnel Syndrome Questions & Answers page.
Anatomy of the Carpal Tunnel
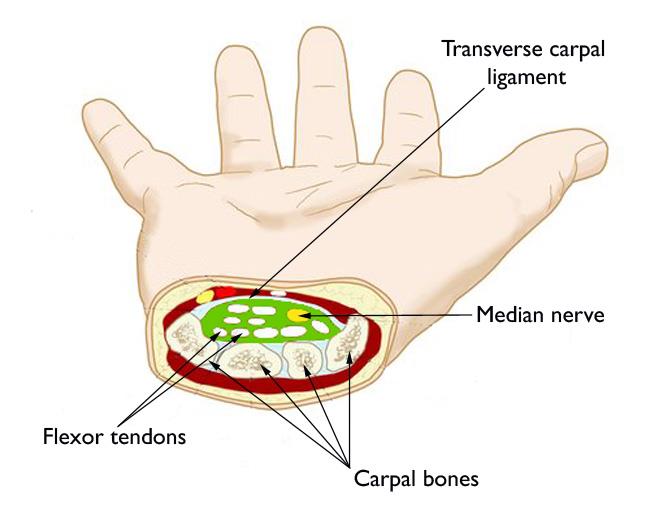
The carpal tunnel is a narrow, rigid passageway located at the base of the palm. It is formed by the carpal (wrist) bones on the bottom and sides, and the transverse carpal ligament — a tough fibrous band — across the top. Within this confined space travel the median nerve and nine flexor tendons responsible for moving the fingers and thumb.
The median nerve is a mixed nerve, meaning it carries both sensory and motor signals. It provides sensation to the thumb, index finger, middle finger, and the radial (thumb) half of the ring finger. It also controls the thenar muscles at the base of the thumb, which control the fine motor movements essential for grip and pinch.
Because the tunnel itself has virtually no capacity to expand, any process that increases pressure within it — whether from swelling, anatomical variation, or inflammation — compresses the median nerve and produces the hallmark symptoms of carpal tunnel syndrome.
Symptoms of Carpal Tunnel Syndrome
Common Sensory Symptoms
- Numbness and tingling in the thumb, index, middle, and part of the ring finger
- Burning or aching pain in the palm, wrist, or forearm
- Nocturnal symptoms — patients are frequently awakened at night by hand discomfort
- A sensation of swelling in the fingers even when none is visible
- Symptoms that worsen with sustained wrist flexion or extension (e.g., driving, reading, typing)
Motor and Functional Symptoms
- Weakness when gripping or pinching objects
- Difficulty with fine motor tasks such as buttoning clothing or handling small items
- Dropping objects unexpectedly due to grip weakness
- Thenar muscle atrophy — visible wasting at the base of the thumb — in advanced or long-standing cases
The severity of your symptoms does not always match what nerve testing shows. Patients with mild nerve conduction abnormalities may report significant functional limitations, and vice versa. Clinical correlation is essential.
Causes and Risk Factors
Structural and Anatomical Factors
- Hereditary predisposition — a congenitally narrowed carpal tunnel significantly increases lifetime risk
- Acute wrist injuries — fractures and dislocations can alter tunnel geometry or cause post-traumatic swelling
- Degenerative arthritis affecting the carpal joints
Inflammatory and Soft Tissue Causes
- Tenosynovitis — inflammation and thickening of the flexor tendon sheaths, which occupy shared space within the tunnel
- Rheumatoid arthritis and other inflammatory arthropathies
- Gout or pseudogout deposits within the tunnel
Systemic and Metabolic Conditions
- Diabetes mellitus — peripheral nerves in diabetic patients are more susceptible to compressive injury
- Thyroid dysfunction, particularly hypothyroidism, which promotes fluid retention and soft tissue swelling
- Pregnancy-related fluid retention — a common, often transient cause of CTS that typically resolves postpartum
- Renal failure and dialysis-related amyloidosis
- Obesity
Occupational and Activity-Related Factors
- Repetitive wrist flexion and extension over prolonged periods
- Prolonged use of vibrating hand tools
- Sustained awkward wrist postures
It is important to note that while occupational factors are frequently cited, the scientific literature does not support repetitive hand use as an independent cause of CTS in the absence of other risk factors.
Diagnosis
Clinical History
Physical Examination
- Sensory testing of median-innervated and non-median-innervated digits to map the distribution of numbness
- Thenar muscle strength assessment — evaluating grip and pinch strength at the base of the thumb
- Phalen's test — sustained wrist flexion for 60 seconds; reproduction of symptoms is a positive finding
- Tinel's sign — percussion over the carpal tunnel at the wrist; tingling in the median nerve distribution is a positive finding
- Two-point discrimination testing — a simple test that measures how well the fingertips can still detect sensation
- Examination of the neck and shoulder region to confirm that symptoms are not originating from a nerve compression elsewhere in the arm
Imaging
X-rays of the wrist are obtained routinely to assess for bony abnormality, fracture malunion, arthritis, or calcified deposits within the tunnel. MRI or ultrasound may be indicated in atypical presentations or when a space-occupying lesion (e.g., ganglion cyst, lipoma) is suspected.
Electrodiagnostic Studies
Nerve conduction studies (NCS) and electromyography (EMG) remain the gold standard for confirming median nerve compression, quantifying its severity, and excluding proximal or generalized neuropathy. These studies measure the speed and amplitude of nerve signals across the carpal tunnel.
Diagnostic Injection
A corticosteroid injection into the carpal tunnel may serve both a therapeutic and diagnostic purpose. Significant symptom relief following injection supports the diagnosis of CTS and may help determine the likelihood of a favorable response to surgical decompression.
Treatment Options
Treatment selection is individualized based on symptom severity, duration, electrodiagnostic findings, patient activity level, and response to prior interventions. As with most orthopedic conditions, a stepwise approach — beginning with conservative measures — is standard of care.
Non-Surgical Treatment
1. Activity Modification
Identifying and reducing activities that require sustained or forceful wrist flexion and extension can significantly reduce symptoms, particularly in patients with occupationally or behaviorally driven CTS.
2. Wrist Splinting
Neutral-position wrist splints minimize pressure within the carpal tunnel by preventing the extremes of flexion and extension. Nocturnal splinting is particularly effective, as most patients involuntarily flex the wrist during sleep — compounding nerve compression and disrupting rest.
3. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
Oral NSAIDs such as ibuprofen or naproxen may reduce perineural inflammation and provide symptomatic relief, particularly in cases with a prominent inflammatory component (e.g., tenosynovitis). They are most useful as an adjunct to other conservative measures rather than as a standalone treatment.
4. Corticosteroid Injection
An injection of a corticosteroid combined with a local anesthetic into the carpal tunnel can provide meaningful symptom relief by reducing inflammation and edema around the nerve. Injections are often effective in the short to medium term and are particularly useful for managing acute flares or as a bridge to definitive surgical treatment. Effects may be temporary, and repeat injections are typically limited to avoid potential tendon or nerve injury.
Surgical Treatment
If conservative treatment fails to provide adequate relief — or if the patient presents with thenar atrophy, persistent motor weakness, or severe electrodiagnostic findings — surgical decompression is indicated. The goal of surgery is to divide the transverse carpal ligament, enlarging the tunnel and relieving pressure on the median nerve.
The procedure is performed on an outpatient basis and takes approximately 10 to 15 minutes under local or regional anesthesia. Dr. Donnelly performs two standard techniques:
Open Carpal Tunnel Release
A small incision is made in the palm, providing direct visualization of the transverse carpal ligament, which is then divided under direct vision. Open release is the time-tested standard approach with an extensive track record of safety and efficacy. Learn more on our Open Carpal Tunnel Release page.
Endoscopic Carpal Tunnel Release
Using a small camera (endoscope) inserted through one or two small incisions, the ligament is divided from inside the tunnel without opening the palm. This minimally invasive technique is associated with less post-operative palmar scar tenderness and, in many patients, a faster return to work and daily activities. Learn more on our Endoscopic Carpal Tunnel Release page.
The choice of technique is determined after a thorough discussion with Dr. Donnelly about your anatomy, occupation, and preferences. Both approaches produce equivalent long-term outcomes when performed by an experienced hand surgeon.
Recovery and Outcomes
Many patients experience rapid relief of numbness and tingling following surgical decompression — often within days of the procedure. However, the pace of recovery is directly related to the severity and duration of nerve compression prior to surgery.
- Mild to moderate CTS: sensory symptoms typically resolve within days to weeks; full recovery is expected
- Severe or long-standing CTS: nerve regeneration takes longer; numbness and tingling may persist for several months, and thenar weakness may improve only partially if significant muscle atrophy was present
- Palmar incision tenderness ("pillar pain") is common and typically resolves within 4 to 8 weeks
- Most patients return to light daily activities within 1 to 2 weeks
- Return to manual or physically demanding work: typically 3 to 6 weeks, depending on the technique used and occupational demands
- Hand therapy may be recommended to optimize strength, range of motion, and scar management
Recurrence following appropriately performed carpal tunnel release is uncommon. Persistent symptoms after surgery most often reflect incomplete ligament division, an incorrect diagnosis, or a pre-existing condition such as diabetic neuropathy that continues to affect the nerve independently.
Additional Resources
For further reading, Dr. Donnelly's patient education library includes the following in-depth resources:
Schedule a Consultation in Greater New Orleans

If you’re experiencing numbness, tingling, or hand weakness, early evaluation can make a significant difference in your recovery. Dr. Donnelly proudly serves patients throughout Greater New Orleans, including Metairie, Covington, Mandeville, and the North Shore.
Call our office or request an appointment online: