
Open Surgery for Wrist Fractures
 Open surgery for wrist fractures is a common treatment for wrist fractures that can not be treated non-operatively. Most wrist fractures occur at the end of the larger forearm bone called the radius, referred to as distal radius fractures. Distal radius fractures come in many different types and patterns, which are often treated differently. They can be treated by immobilizing the wrist in a cast or splint, or operatively by performing a procedure called “open reduction internal fixation” (ORIF).
Open surgery for wrist fractures is a common treatment for wrist fractures that can not be treated non-operatively. Most wrist fractures occur at the end of the larger forearm bone called the radius, referred to as distal radius fractures. Distal radius fractures come in many different types and patterns, which are often treated differently. They can be treated by immobilizing the wrist in a cast or splint, or operatively by performing a procedure called “open reduction internal fixation” (ORIF).
Non-displaced or minimally displaced fractures are often amendable to non-surgical treatment. A cast or brace is used for 4-6 weeks until the bone heals. These are followed closely with x-rays over the first 2-3 weeks to make sure the fracture does not displace.
Open surgery for wrist fractures is often required for displaced fractures. This allows better alignment of the fracture and early motion of the wrist as rigid casts are seldom needed. The wrist is the foundation for the hand, and as such, poor alignment of wrist fractures can lead to continued pain, arthritis, finger stiffness and compromised hand function.
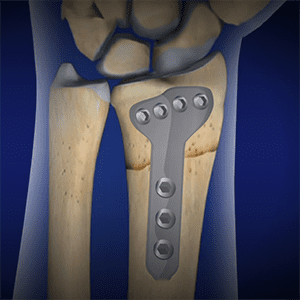
There are several techniques for surgical fixation of distal radius fractures but most often is with an open incision and plate and screw fixation.
What are the Risks of Open Surgery for Wrist Fractures?
The most common risk of distal radius fracture is stiffness and loss of motion of the wrist. Fortunately, this loss of motion is usually less than 10-15 degrees and the wrist maintains full function. This can happen in both surgical and non-surgical fractures.
Routinely the bone will heal, even without surgery, but when it does not it is referred to as a nonunion. Nonunion of distal radius fractures is uncommon, but can be associated with open or “compound” fractures, gross malalignment, vitamin deficiency (Vitamin D and Calcium), diabetes and other system illness. Again, this can happen with or without surgery. A malunion occurs when the bone heals, but is maligned. This is much more common in non-surgically treated fractures, and in more severe cases can impair function.
Risks particular to surgery, although rare, include infection, bleeding, scarring, hardware prominence, and possible injury to nerves, vessels, or tendons.
What is a Distal Radius ORIF Procedure?
A distal radius ORIF is a 30-90-minute outpatient surgery that is typically performed under either general anesthesia or regional “nerve block” anesthesia. After the patient is comfortable and asleep, the procedure is performed through the following steps:
- An incision is made on the palm side of the forearm and wrist.
- Surgical instruments are used to access the wrist and view the fracture.
- The fracture is realigned and a combination of a plate and multiple screws are placed to secure the fracture position.
- The incision is closed using sutures and a plastic surgery technique to limit scarring.
Dressings are placed over the incision and a splint that extends from the mid forearm to the palm is placed over the dressings and secured with light bandage. The elbow and fingers are left free to allow motion.
What happens after the procedure?
The goal the first week after surgery is to control swelling and pain. This is accomplished through elevation of the extremity and icing. Pain medicine and anti-inflammatories are also utilized. Another key this first week is start finger motion, to prevent stiffness.
The first postoperative appointment occurs 1-2 weeks after surgery. Sutures are typically removed at this time. Depending on the severity of the injury, removable splint, or less often, a cast, is used for protection. Patients are encouraged to continue to move their fingers and elbow. Light wrist motion is often started at this time but no significant lifting or gripping with the arm is allowed. “You can move it, but can’t use it.”
Hand therapy may be started after surgery. Hand therapy is similar to physical therapy, but incorporates distinct techniques geared toward the intricate function of the hand and wrist.
The brace is discontinued 4-6 weeks after surgery and increasing activities are allowed. It is important to note that not all fractures heal in the same amount of time. Bone healing depends on fracture severity and the healing processes of the patient. Factors that can decrease healing include co-morbid conditions such as diabetes and tobacco/nicotine use.
Return to unrestricted activity is around 8-10 weeks after surgery. However, discomfort may linger for 3-6 months after surgery, as the soft tissues and ligaments take longer to heal than the bone.